.svg)
Share this post

How US Healthcare Companies Are Using Offshore SDRs to Break Into New Market Segments in 2026
US healthcare companies are under pressure from every direction. Customer acquisition costs are rising. Existing accounts face more competition. And the board wants pipeline growth without a proportional headcount budget to match.
The answer a growing number of healthcare sales leaders are finding: dedicated offshore SDRs deployed specifically to penetrate new market segments, not as a cost-cutting measure, but as a genuine growth strategy.
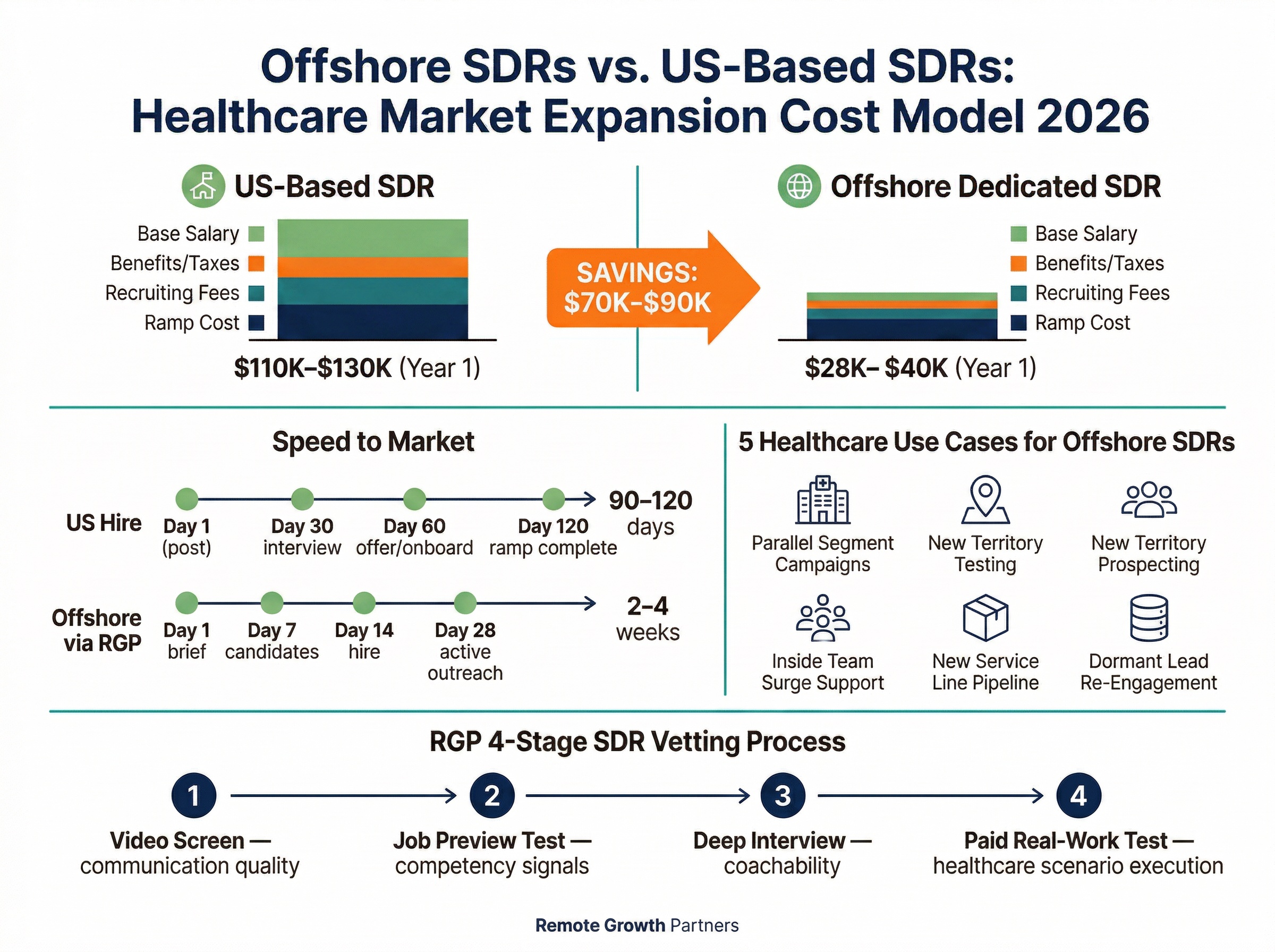
Quick Answer: US healthcare companies use dedicated offshore SDRs to run simultaneous prospecting campaigns across new buyer segments, test new geographic territories before committing to full-time US hires, and build top-of-funnel pipeline for new product lines, all at 40–60% lower cost than a domestic SDR hire. The key is pairing a fully-vetted, dedicated offshore SDR with a documented outreach playbook built specifically for the target segment.
Key Takeaways:
- Dedicated offshore SDRs let healthcare organizations launch new market segment campaigns in 3–4 weeks, vs. 90+ days for a US hire.
- A fully managed offshore SDR costs $28K–$40K/year all-in, compared to $110K–$130K fully loaded for a US-based SDR in Year 1.
- The $70K–$90K cost delta funds additional offshore SDRs, paid outreach, or content, amplifying the new segment push.
- Healthcare organizations using offshore SDRs for market expansion succeed when the ICP, messaging, and outreach playbook are defined before the hire starts.
- Remote Growth Partners places dedicated (not shared) offshore SDRs through a 4-stage vetting process that includes a paid real-work test specific to each client's target segment.
The 2026 Pressure Point: Why Healthcare Organizations Can't Afford to Ignore New Market Segments
Healthcare B2B sales has gotten harder. That's not an opinion, the data backs it up.
The Pipeline Problem Facing Healthcare Sales Teams Right Now
According to research published by the Healthcare Financial Management Association ↗, procurement cycles in hospital systems have lengthened, with more stakeholders involved in purchasing decisions than at any point in the last decade. Simultaneously, venture-backed health tech competitors are flooding existing segments with aggressive outbound campaigns and discounted trial offers, eroding the relationship advantages that established vendors once relied on.
The practical effect: your existing SDR team is fighting harder to maintain pipeline in segments they already know, leaving no bandwidth to develop new ones.
"The healthcare organizations growing fastest in 2026 are not the ones with the biggest sales teams, they're the ones running parallel prospecting motions across multiple buyer segments simultaneously."
That's the core strategic insight. When your US-based reps are protecting existing accounts and closing active deals, who is building the pipeline in adjacent markets?
Why Traditional Hiring Can't Keep Up With Market Expansion Goals
A US-based SDR hire takes 60–90 days to source, screen, and onboard. Add a 60-day ramp period before they're operating at full capacity, and you're looking at 5–6 months before meaningful pipeline emerges from a new segment. At an average fully loaded cost of $110K–$130K in Year 1 (we'll break this down in detail later), that's a significant bet on an unproven market.
Most healthcare sales leaders don't make that bet. They wait until the segment proves itself, but the segment can't prove itself without outreach. It's a circular problem.
Offshore SDRs break the circle. Healthcare organizations deploy offshore SDRs to generate pipeline validation data in new segments before committing to the full cost of a domestic hire. That's not corner-cutting. That's intelligent market testing.
What 'New Market Segment Penetration' Actually Means for a Healthcare Sales Org
Before talking strategy, it's worth being precise about what "new market segment" means in practice. Healthcare B2B sales leaders use the phrase to mean three distinct things, and each has different offshore SDR implications.
Geographic Expansion: Reaching New US Regional Markets
This is the most straightforward case. A healthcare SaaS company that has solid penetration in the Northeast wants to build pipeline in the Mountain West or Southeast. The target buyers are the same type (hospital procurement teams, health system CFOs), just in a different geography.
Healthcare organizations use offshore SDRs for geographic expansion because the prospecting motion is already documented. The ICP is known. The messaging is tested. You're just running the same playbook in a new zip code, and an offshore SDR can do that without a full US-based hire in a region where you have no office presence.
Vertical Expansion: Moving Into Adjacent Healthcare Buyer Personas
This is more complex and more common among growth-stage healthcare companies. You've sold into large hospital systems. Now you want to move into ambulatory surgery centers (ASCs), urgent care chains, behavioral health networks, or independent physician groups. These are adjacent buyer personas, they exist in the same industry, but they have different budgets, different decision-making structures, different pain points, and different objection patterns.
Healthcare organizations use offshore SDRs for vertical expansion to run a dedicated outbound motion for the new persona without pulling existing reps off their productive hospital-system pipeline. The offshore SDR becomes the specialist for the new segment, while your US team keeps operating in the segment they know.
Product Line Expansion: Promoting New Services or Solutions to Existing Networks
The third scenario is one many healthcare organizations overlook: you have a new product, service line, or solution, and you need dedicated outreach capacity to build awareness without cannibalizing your existing AE pipelines. Your account executives shouldn't be prospecting cold contacts for a new product while managing active deal cycles. Healthcare organizations use offshore SDRs to create top-of-funnel capacity for a new product launch without disrupting existing revenue motions.
Why Offshore SDRs Are Uniquely Suited to Healthcare Market Expansion
Not every sales function translates cleanly to an offshore model. But SDR work, targeted outbound prospecting, sequence execution, meeting booking, and pipeline handoff, is highly structured, measurable, and geography-independent. Here's why offshore SDRs specifically fit the market expansion use case.
Speed to Market: From Decision to Active Outreach in Weeks, Not Months
Remote Growth Partners can typically place a dedicated offshore SDR within 2–4 weeks of a client engagement. That's not a claim, it's a function of maintaining a pre-vetted candidate pipeline across Latin America, the Philippines, and Eastern Europe. Compare that to the 60–90 day US hiring cycle, and the calculus is obvious.
For healthcare organizations trying to launch a new segment campaign in Q3 while budget is available, speed is not a nice-to-have. It's the whole game.
Cost Efficiency That Lets You Test Multiple Segments Simultaneously
At $28K–$40K/year fully managed, a dedicated offshore SDR costs less than one-third of a fully loaded US hire. That means a healthcare organization with a $120K annual budget can fund one US SDR or three offshore SDRs testing three different segments simultaneously. One of those segments shows conversion. You scale into it. The other two didn't work. You've spent $40K to find that out rather than $120K plus 6 months of your team's time.
Scalability Without the Risk of Locking In High Fixed Costs
US hires come with fixed costs that are hard to unwind quickly: base salary commitments, benefits, equity, severance considerations. Offshore SDRs through a managed service model like Remote Growth Partners are structured as a dedicated full-time engagement, with the flexibility to scale up or restructure as market data comes in.
Dedicated Focus: One SDR, One Segment, One Mission
This point matters more than it sounds. Shared offshore SDRs (common on generalist platforms) split their attention across multiple clients. That's not acceptable for new market penetration work, which requires deep familiarity with a specific ICP, specific messaging, and a specific segment's objection patterns.
Remote Growth Partners places dedicated offshore SDRs, one client, full-time, no sharing. That means the SDR builds genuine expertise in your target segment over time, which compounds in ways that shared attention never does.
5 Ways US Healthcare Companies Are Using Offshore SDRs to Break Into New Markets in 2026
1. Running Parallel Prospecting Campaigns Across Multiple Buyer Segments
A healthcare SaaS company selling revenue cycle management (RCM) software has its US team focused on enterprise hospital system procurement teams. The VP of Sales wants to test whether independent physician groups (IPGs) represent a viable adjacent market, but pulling an existing rep off the hospital motion would risk active deal cycles.
The solution: deploy a dedicated offshore SDR to run a simultaneous campaign targeting IPG office managers and practice administrators. The offshore SDR works a list of 1,500 contacts, runs a 6-touch email and LinkedIn sequence, and handles initial discovery calls. By Week 10, there are 22 booked meetings with IPGs, enough data to validate the segment and justify a dedicated US-based AE.
Healthcare organizations run parallel prospecting campaigns using offshore SDRs so that new segment testing never comes at the cost of existing segment performance.
2. Testing New Geographic Territories Before Committing to a Full US-Based Hire
A medical device company selling orthopedic surgical tools has strong penetration in the Midwest. Leadership wants to expand into the Pacific Northwest, a territory that would normally require a US-based field rep at $90K+ base salary plus car, travel, and benefits.
Before that commitment, they deploy an offshore SDR to run a 90-day outbound campaign targeting OR directors and surgical procurement managers in the target geography. The SDR books 15 discovery calls, which convert to 6 qualified demos. The pipeline generated justifies the field hire. The total cost of the validation phase: $10K.
That's the math that makes offshore SDR geographic testing compelling.
3. Supplementing an Existing Inside Sales Team During Capacity Crunches
Q3 is a pressure cooker for many healthcare companies. Existing inside sales reps are deep in deals trying to hit mid-year quota. Top-of-funnel activity, the cold outreach that builds Q4 and Q1 pipeline, falls off a cliff.
A health tech company used an offshore SDR as a temporary capacity supplement during exactly this window: six months of dedicated top-of-funnel outreach while the inside team focused on closing. The offshore SDR ran 4 sequences simultaneously, covering two new verticals (behavioral health networks and telehealth platforms). By the end of Q3, the company had 40+ new contacts in active pipeline sequences, none of which would have existed if the inside team was relied upon to generate them while under quota pressure.
4. Building Top-of-Funnel Pipeline for a New Product or Service Line
A healthcare consulting firm launches a new managed care contracting service targeting regional health plans. Their existing AEs know the buyer (health plan medical directors and contracting VPs), but there's no playbook, no contact list, and no established message for the new service.
Rather than task existing AEs with cold prospecting while managing client relationships, the firm hires a dedicated offshore SDR specifically to build the top-of-funnel motion from scratch. The SDR builds the contact list, tests three different email angles over 60 days, identifies which message lands, and begins booking discovery calls. By month 3, the new service has its own pipeline, separate from the AE team's existing workload.
Healthcare organizations use offshore SDRs for new product launches to protect AE bandwidth while generating the initial pipeline data needed to refine positioning.
5. Re-Engaging Dormant Accounts and Stale Leads at Scale
Healthcare staffing companies often accumulate large databases of contacts who engaged at some point but went cold. A 2,000-contact lapsed lead database has real value, but re-engagement campaigns require volume and consistency that busy inside teams rarely prioritize.
A healthcare staffing company deployed an offshore SDR exclusively to work a dormant database of 2,200 past prospects across hospital networks and long-term care facilities. Using a personalized 5-touch re-engagement sequence, the SDR generated 34 responses and 19 booked calls in the first 60 days. Total pipeline reactivated: estimated $1.8M in potential placement fees.
That's value that was sitting in the CRM, generating nothing.
How to Structure an Offshore SDR for Maximum Market Penetration Impact
Healthcare organizations that get the most out of offshore SDR market expansion share one common trait: they invest in the setup before the hire starts. Here are the five steps that separate high-performing deployments from expensive disappointments.
Step 1: Define the Target Segment With Surgical Precision Before Hiring
What to do: Before you post the role or start the vetting process, write a one-page segment definition. It should include: the specific buyer persona (title, organization type, size), the geography, the pain point you're solving for them, and the reason they'd take a 15-minute call with an unknown vendor.
Why it matters for market expansion: The offshore SDR is executing a segment-specific mission. Without a precise definition, they will default to generic outreach, which wastes their time and yours. Vague ICPs produce low reply rates and low booking rates. A tight ICP produces 3× better engagement.
Practical healthcare example: Instead of "target hospital purchasing managers," your definition might read: "Director of Supply Chain at community hospitals (100–300 beds) in the Southeast US, dealing with vendor consolidation pressure and facing contract renewal season in Q3."
That is an ICP an offshore SDR can actually work.
Step 2: Choose the Right Offshore Region for Your Target Market
What to do: Match the offshore SDR's region to the needs of your campaign. The three main options are Latin America (LATAM), the Philippines, and Eastern Europe, each with different cost profiles, time zone alignment, and communication styles.
Why it matters: Time zone alignment is critical for cold calling. If your target buyers are in US Eastern or Central time zones, LATAM (particularly Colombia, Mexico, and Argentina) offers same-day working hour overlap. The Philippines aligns better for email-heavy or async-first campaigns. Eastern Europe (Poland, Romania) works well for campaigns that need strong written communication skills and can tolerate a partial time zone overlap.
For a full breakdown of regional tradeoffs, see our guide on the best countries to hire offshore SDRs in 2026.
Step 3: Build a Segment-Specific Outreach Playbook Before Day One
What to do: Deliver a complete, written playbook to the offshore SDR before they make their first contact. A functional playbook for healthcare market expansion includes:
- ICP definition (detailed, as above)
- Messaging by persona, different messages for clinical buyers vs. Administrative buyers vs. Finance buyers
- Objection handling, the 5–7 most common objections and scripted responses
- CRM workflow, exactly how to log calls, tag records, update stages, and escalate hot leads
- Call scripts, full scripts for cold calls, voicemail scripts, and follow-up calls
- Email cadence templates, minimum 6-touch sequence with subject lines, body copy, and send timing
- LinkedIn outreach templates, connection request copy and follow-up messaging
Why it matters: This is not hand-holding. It's infrastructure. The playbook is how your offshore SDR executes your strategy, not theirs. Healthcare buyers are skeptical of unsolicited outreach, the messaging has to be precise, credible, and segment-specific. A generic sequence will produce 0.5% reply rates. A well-built playbook for a specific healthcare persona can produce 4–8%.
For a complete template, see the 30-day offshore SDR onboarding playbook.
Step 4: Set Up the Right Tech Stack for Smooth Remote Operation
What to do: Provision the SDR with the tools they need before Day 1. Minimum viable stack for a healthcare outbound SDR campaign: a CRM (HubSpot or Salesforce), a sequencing tool (Apollo, Outreach, or Salesloft), a calling solution (Aircall or Dialpad), LinkedIn Sales Navigator, and a shared Slack or Teams channel for real-time communication.
Do not assume the SDR will "figure out" the tools. Create a written tool guide with login instructions, how you want data entered, and who they contact when something breaks. This takes two hours to build and saves weeks of confusion.
Step 5: Define Success Metrics for the First 30, 60, and 90 Days
What to do: Set explicit, written benchmarks before the engagement starts. A reasonable set for a new healthcare market segment:
- Day 30: 300+ contacts loaded and sequenced, initial messaging performance data (open rates, reply rates), first calls attempted
- Day 60: 15–20 conversations with target buyers, 5+ booked discovery meetings, messaging refinement based on objection patterns
- Day 90: 10+ qualified meetings delivered to AE pipeline, segment conversion data available to inform hiring and scaling decisions
Why it matters: Without defined metrics, performance reviews become subjective. With them, you can identify at Day 30 whether messaging needs adjustment, at Day 60 whether the SDR needs coaching, and at Day 90 whether the segment warrants scaling.
According to SHRM research on sales role performance ↗, organizations that set explicit 30/60/90-day performance benchmarks for new hires see 23% higher retention and significantly faster time-to-productivity, a finding that applies equally to offshore sales roles.
What Healthcare Organizations Get Wrong When Scaling With Offshore SDRs
Remote Growth Partners works with healthcare companies at every stage of offshore SDR adoption. When clients come to us after a previous offshore SDR attempt that didn't work, the failure pattern is almost always one of four things.
Mistake 1: Hiring Before the Playbook Is Ready
The most common failure mode is not the SDR, it's the absence of a defined ICP and a tested message before the hire begins. Organizations bring on an offshore SDR expecting them to generate pipeline from day one, with nothing but a product overview deck and a vague target list. The SDR does their best with what they have, sends generic emails, gets poor response rates, and gets labeled "not effective." The playbook was never built. The SDR never had a chance.
Mistake 2: Expecting the SDR to Define the ICP
A related but distinct mistake: hiring an offshore SDR and asking them to figure out who to target and what to say. ICP definition and message development are strategy functions, not execution functions. The SDR's job is to execute a documented strategy with high volume and consistent follow-through. If you don't have the strategy documented, you don't have an SDR problem, you have a strategy problem. Solve the strategy problem first.
Mistake 3: Treating Offshore Like a Second-Class Team Member
Healthcare organizations that get the best results from offshore SDRs include them in team meetings, give them a named Slack presence, introduce them to AEs they'll be handing leads to, and celebrate their wins publicly. Organizations that treat the offshore SDR as a vendor (rather than a team member) consistently see lower performance, higher turnover, and weaker alignment with company culture.
The SDR is not a contractor. They're a dedicated full-time member of your revenue function who happens to be based in a different country.
Mistake 4: Not Tracking the Right Leading Indicators
Booked meetings are a lagging indicator. By the time you have booking data, four weeks of outreach have already happened. The leading indicators that tell you whether a new market segment campaign is working, and that you should be watching from Week 1, are:
- Sequence open rates (above 35% is healthy for cold outreach)
- Reply rates (2–4% for cold email is a reasonable baseline; anything above 6% signals strong message-market fit)
- Connect rates on cold calls (10–15% is typical; below 8% suggests list or time-of-day issues)
- Objection patterns (what are buyers saying when they reply negatively? This is market intelligence, not just a metric)
If you're only looking at meetings booked, you're flying blind for the first 30 days of every campaign.
Real Cost Model: Scaling Healthcare Pipeline With Offshore SDRs vs. US Hires in 2026
Total Cost of a US-Based SDR for New Market Expansion
| Cost Component | Estimate |
|---|---|
| Base salary | $60,000 – $75,000 |
| Benefits and payroll taxes (25%) | $15,000 – $18,750 |
| Recruiting fees (one-time) | $5,000 – $10,000 |
| Equipment and software | $3,000 – $5,000 |
| 60-day ramp at 50% productivity (cost of lost output) | $10,000 – $15,000 |
| Manager time for hiring and onboarding | $5,000 – $8,000 |
| Total Year 1 Fully Loaded Cost | $98,000 – $131,750 |
Total Cost of a Dedicated Offshore SDR for New Market Expansion
| Cost Component | Estimate |
|---|---|
| Fully managed annual placement (salary, payroll, compliance, account management) | $28,000 – $40,000 |
| Equipment/software provisioning | $1,500 – $3,000 |
| Playbook and onboarding investment (internal) | $1,000 – $2,500 |
| Total Year 1 Fully Loaded Cost | $30,500 – $45,500 |
What the Cost Difference Allows You to Do Strategically
The gap between a US SDR and a dedicated offshore SDR is $68K–$86K per year. That budget does not disappear, it becomes strategic fuel.
With the cost savings from one offshore SDR vs. a domestic hire, a healthcare organization can fund a second offshore SDR targeting a different segment, a $20K paid media budget to amplify the outbound campaign, or content production for segment-specific sales enablement materials, all simultaneously.
Options for redeploying the $70K–$90K delta:
- Fund 2–3 additional offshore SDRs to test additional segments in parallel
- Invest in paid LinkedIn or programmatic outreach to the same segment the SDR is calling
- Build segment-specific case studies, one-pagers, and video assets for the SDR to reference in outreach
- Hire a fractional revenue operations resource to build out CRM infrastructure for the new segment
This is not about going cheap on headcount. It's about deploying capital in a way that actually tests the market before you over-invest in it.
The Vetting Factor: Why Not All Offshore SDRs Deliver the Same Expansion Results
The offshore SDR market is not uniform. There's a significant performance gap between a candidate who was quickly placed through a generalist staffing platform and a candidate who went through a rigorous, role-specific vetting process. For healthcare market expansion, where the buyer is sophisticated, the message needs to be credible, and the first impression can close a door permanently, vetting is not optional.
What a 4-Stage Vetting Process Looks Like for Healthcare SDR Candidates
Remote Growth Partners uses a 4-stage vetting process for every offshore SDR candidate. Here's what each stage filters for:
Stage 1: Video Screen
The initial video screen assesses communication quality, professional presentation, and English fluency, the table stakes for US healthcare outreach. Candidates who pass this stage present clearly, maintain eye contact, speak at a natural pace, and demonstrate the composure that healthcare buyers expect in a first-call interaction.
Stage 2: Job Preview Test
Candidates complete a role-specific competency assessment. For SDR roles, this tests cold calling and email writing fundamentals, CRM proficiency, and scenario-based problem solving. This stage eliminates candidates who can talk about prospecting but can't execute it.
Stage 3: Deep Interview
This is a structured interview that assesses motivation, coachability, and healthcare sales context awareness. We want to know: Does this candidate understand what it means to prospect into a hospital procurement team? Do they understand why a medical device sale is different from a SaaS sale? Can they receive feedback and apply it quickly? Coachability matters more than experience for new segment work, because the SDR will be learning the vertical as they go.
Stage 4: Paid Real-Work Test
Candidates complete a client-specific task using materials provided by RGP. For healthcare SDR roles, this typically means: write a 3-email cold outreach sequence for a specific product targeting a specific buyer persona. The instructions are realistic and the task mirrors the actual work.
To learn more about how this process works, see how Remote Growth Partners vets offshore SDR candidates.
Why a Paid Real-Work Test Is the Most Predictive Signal for Market Expansion Success
Every other stage of vetting tests potential. The real-work test measures execution. For new market segment work specifically, the real-work test surfaces whether a candidate can adapt their approach to an unfamiliar vertical, which is exactly what they'll be doing when they start.
A candidate who writes a generic, feature-heavy cold email for a hospital CMO has not yet internalized how healthcare buyers think. A candidate who writes a problem-first email that references a real pain point in clinical operations, keeps it under 100 words, and includes a specific, low-friction call to action, that candidate has the signal we're looking for.
Red Flags in Offshore SDR Hiring That Signal Future Market Penetration Failure
If you're vetting candidates yourself, watch for:
- Candidates who can't explain why a specific buyer persona cares about your product
- Candidates whose writing samples are template-heavy and impersonal
- Candidates who have never used a CRM or sequencing tool
- Candidates who struggle to handle a basic objection in a role-play scenario
- Candidates who ask for excessive clarity before starting any task, in market expansion work, some ambiguity is inevitable and candidates need to move through it, not wait for it to resolve
How to Know When You're Ready to Scale With a Second or Third Offshore SDR
Scaling offshore SDRs too early is as costly as scaling too late. Here is the decision framework for when to add headcount to a new segment effort.
Leading Indicators That Your First Offshore SDR Hire Is Working
Before adding a second SDR, your first hire should be consistently hitting:
- 3+ booked meetings per week by Week 8 of active outreach
- Outreach sequences that are documented and repeatable, the SDR should be able to train someone else on the process
- Segment conversion rate at ≥50% of your existing segment's benchmark, new segments will naturally convert lower, but you want evidence they're converting, not just that conversations are happening
If all three of these are present by Week 10–12, the segment is viable and the SDR's motion is working. That's your green light to add capacity.
How to Systematize What's Working Before You Scale
Before hiring SDR #2, document:
- The exact ICP that is converting (not the original broad ICP, the refined version based on 60 days of data)
- The email and call sequences that are driving replies and conversions
- The objections that kill deals and the responses that resolve them
- The CRM workflow, exactly how contacts are entered, staged, and handed to AEs
- The onboarding process for the new SDR (based on what you wish you had given SDR #1)
This documentation turns a single successful SDR into a repeatable process. Without it, every new hire starts from scratch.
Building a Scalable Offshore SDR Team Structure for Healthcare
As the segment matures, the offshore SDR team can evolve from a single contributor to a structured unit:
| Role | Typical Timeline | Primary Responsibility |
|---|---|---|
| Offshore SDR | Months 1–8 | Segment penetration, meeting booking, CRM maintenance |
| Senior Offshore SDR | Months 8–18 | Higher-value accounts, AE coordination, sequence refinement |
| Offshore SDR Team Lead | 18+ months | Coaching junior SDRs, reporting, playbook ownership |
This structure mirrors what you'd build with a US-based SDR team, at a fraction of the fixed cost. If you're considering building this kind of structure, hire a dedicated offshore sales rep for your healthcare team and start the conversation about longer-term team architecture from the beginning.
Before signing with any provider, also check out 15 questions to ask a sales outsourcing company before signing, it will save you from a lot of avoidable mistakes.
Summary
Healthcare organizations using offshore SDRs for market expansion can deploy dedicated outreach capacity into new buyer segments in 2–4 weeks at a fully loaded annual cost of $30,500–$45,500, compared to $98,000–$131,750 for a US-based hire. Offshore SDR healthcare market expansion works best when the ICP, outreach playbook, and success metrics are defined before the hire starts, not after. The five primary use cases in healthcare are: parallel prospecting across multiple buyer personas, geographic territory testing, inside team capacity supplementation, new product line pipeline building, and dormant database re-engagement. Remote Growth Partners places dedicated, fully managed offshore SDRs through a 4-stage vetting process including a paid real-work test that predicts new segment performance more accurately than interviews alone. Healthcare sales leaders scaling with offshore SDRs should look for 3+ booked meetings per week by Week 8 as the primary indicator that a segment is viable and ready for headcount expansion.
Frequently Asked Questions: Offshore SDRs and Healthcare Market Expansion
Q: How can offshore SDRs help a healthcare company enter a new market segment?
Healthcare organizations use offshore SDRs to run high-volume, segment-specific outbound campaigns without pulling existing reps off productive accounts. Offshore SDRs handle cold outreach, sequence execution, and initial discovery calls for a new buyer persona or geography, generating pipeline validation data before the company commits to a full domestic hire. The dedicated focus model (one SDR, one segment) allows the new segment motion to build momentum without competing for attention with existing quota targets.
Q: What does it actually cost to scale a healthcare sales team with offshore SDRs in 2026?
A fully managed dedicated offshore SDR through Remote Growth Partners runs $28,000–$40,000 per year, inclusive of salary, payroll, compliance, and account management. Total Year 1 cost including equipment and onboarding runs $30,500–$45,500. Compare that to $98,000–$131,750 fully loaded for a US-based SDR, and the delta ($52,000–$86,000) represents capital that can fund additional SDRs, content, or paid amplification for the same segment.
Q: How quickly can an offshore SDR be deployed for a new healthcare market campaign?
With a pre-vetted candidate pipeline, Remote Growth Partners typically places a dedicated offshore SDR within 2–4 weeks of a client engagement. Active outreach can begin within the first week of placement, assuming the outreach playbook and tech stack are ready. Compare this to the 60–90 day sourcing timeline plus 60-day ramp period for a US SDR hire, and offshore deployment is roughly 4–5 months faster to first meeting.
Q: What healthcare buyer personas are best suited for offshore SDR outreach?
Offshore SDRs perform well across most healthcare administrative and operational buyer personas: hospital supply chain directors, health system CMOs and CFOs (for initial meeting booking), practice administrators, ASC directors, long-term care facility administrators, health plan contracting VPs, and healthcare IT procurement managers. Outreach to clinical buyer personas (physicians, nurses) typically requires more specialized clinical knowledge and may benefit from closer onboarding investment. For a full overview of offshore roles available for healthcare organizations, the range of addressable buyers is broad.
Q: What KPIs should you track when using offshore SDRs for healthcare market expansion?
Track these in order of timing: Week 1–2: sequences loaded, contacts per day. Week 3–4: open rates (target >35%), reply rates (target >2%). Month 2: connect rate on calls (target 10–15%), conversations per week (target 8–12), booked meetings per week (target 3+). Month 3: qualified opportunities handed to AEs, segment conversion rate vs. benchmark. Trailing metrics like pipeline value and closed-won deals become meaningful after Month 4.
Q: What is the difference between using offshore SDRs and a healthcare sales outsourcing agency for new market entry?
A sales outsourcing agency provides shared, multi-client SDRs who split their time across several accounts simultaneously. A dedicated offshore SDR is a full-time resource assigned exclusively to your team, your segment, and your CRM. For new market penetration work, where consistency, relationship memory, and deep segment knowledge compound over time, dedicated beats shared in almost every case. For a fuller comparison, see our ranking of the best sales outsourcing companies ranked for 2026.
Q: How do you onboard an offshore SDR who has never sold in your specific healthcare vertical?
Start with a 5-day orientation that covers: your product or service, the target buyer's world (their day, their priorities, their pain), the competitive space, and the outreach playbook in detail. Follow with daily 15-minute check-ins for the first two weeks to catch confusion early. By Week 3, move to weekly reviews focused on performance metrics. The SDR will not know everything on Day 1, but with a structured playbook and active coaching, most dedicated offshore SDRs hired through a rigorous vetting process are generating qualified meetings within 30–45 days.
Q: How many offshore SDRs do you need to penetrate a new healthcare market segment?
One well-supported offshore SDR is sufficient to validate a new segment in 60–90 days. If the first SDR reaches 3+ booked meetings per week by Week 8, the segment is viable, and that is the right time to consider adding a second SDR to accelerate penetration. For large geographic territories or multiple sub-personas within a vertical (e.g., large hospital systems and community hospitals within the same segment), two SDRs from the start can compress the validation timeline. Start with one, prove the motion, then scale.
Ready to Launch Your Next Market Segment?
The healthcare organizations gaining ground in 2026 are not waiting for their existing pipeline to get easier. They're building parallel prospecting motions into adjacent markets right now: with offshore SDRs that cost a fraction of a domestic hire and can be active in weeks.
If you're a VP of Sales or CRO at a healthcare organization looking to test a new buyer persona, geographic market, or product line without the overhead of a US hire, the math is worth running.
Get started with an offshore SDR placement and see what a dedicated offshore SDR can do for your next market segment. Or read what healthcare sales leaders say about RGP before you decide.
.jpg)
.jpg)
